Ling Zhang, MD,1,* Lei Wu, MD,2,* Xiaolong Xu, PhD,3,* Yadong Yuan, MD,4 Rongmeng Jiang, MD,5 Xixin Yan, MD,4 Xin Zhang, MD,1 Yong Gao, MD,1 Huanxia Shang, MD,1 Jing Hu, PhD,3
Xuerui Wang, MS,3 Jianqiang Mei, MD,2 Shucai Wu, MD,1 and Qingquan Liu, MD3Abstract
Background: Asymptomatic patients are unneglected sources in propagating transmission chain due to their high viral loads. However, treatments available based on symptoms seem not applicable to asymptomatic patients. In this study, the authors want to estimate the effectiveness of Lianhua Qingwen (LH) capsule on asymptomatic coronavirus disease 2019 (COVID-19) patients.
Methods: A randomized controlled trial (RCT) was performed to explore the effectiveness and safety of LH capsule in treating asymptomatic COVID-19 patients. Patients were randomized to control group (isolated observation) and treatment group (LH, 4 capsules, thrice daily) for 14 days. The primary endpoints were the rate and time of nucleic acid turning negative during the isolation observation.Results: A total of 120 participants were included in the full analysis set (60 each in the control and treatment groups). Data showed that the rate of nucleic acid turning negative during the isolation observation in the treatment group was higher than that in the control group (rate difference: 21.66%, 95% confidence interval [CI]: 4.34 to 37.27, p = 0.0142). Patients in the treatment group have a shorter time of nucleic acid turning negative (7.5 vs. 14.5 days, p = 0.018). Moreover, the rate of clinical symptoms appearance in the treatment group was lower compared with that in the control group (rate difference: -31.67, 95% CI: -46.83 to -13.82, p = 0.0005). The proportion of confirmed mild and common cases in the treatment group was also lower (35.00% vs. 66.67%, p = 0.0005). No serious adverse events were documented.
Conclusions: In this study, the authors illustrated that LH capsule is beneficial to asymptomatic COVID-19
patients. Considering the lack of interventions for treating asymptomatic COVID-19 patients at this stage, LH capsule could be considered as a choice.
Chinese Clinical Trial Registry: ChiCTR2100042066.
Keywords: COVID-19, asymptomatic patients, Lianhua Qingwen, effectiveness, clinical trial
1Respiratory Department, Hebei Chest Hospital, Shijiazhuang, P.R. China.
2Respiratory Department, Hebei Hospital of Traditional Chinese Medicine, Shijiazhuang, P.R. China.
3Intensive Care Unit, Beijing Hospital of Traditional Chinese Medicine, Capital Medical University, Beijing, P.R. China.
4Infectious Disease Department, The Second Hospital of Hebei Medical University, Shijiazhuang, P.R. China.
5Infectious Disease Department, Beijing Ditan Hospital, Capital Medical University, Beijing, P.R. China.
*These co-first authors contributed equally to this study.
Introduction
The coronavirus disease 2019 (COVID-19) pandemic
has spread globally since 2019, mainly through human- to-human transmission, and contributes to a major public health problem.1 To date, the public data from the World Health Organization (WHO) showed that severe acute re- spiratory syndrome coronavirus 2 (SARS-CoV-2) has in- fected more than 200 million people with 4 million confirmed deaths. Due to limited pharmaceutical treatments for COVID-19, interventions have to rely more on contact trac- ing, quarantine, and social distancing. Considering the rapid spread and unpredicted variations of SARS-CoV-2, the total incidence of COVID-19 illness will maintain high in the next 5 years and has a chance to enter into a regular circulation.2 This is no doubt a huge challenge for our medical systems, especially the intensive care unit (ICU) capacity. Therefore, developing more complementary interventions to reduce ICU demand is of great importance.3
Initially, COVID-19 patients were generally classified into
four types in China, including mild, common, severe, and critical cases,4 which attract most attentions and medical sources. However, growing case reports documented patients who were positive in polymerase chain reaction (PCR) test but showed no typical clinical symptoms or signs.1,5 With in- depth understanding of the pathogenesis and epidemiology of SARS-CoV-2, asymptomatic COVID-19 patients have been recognized as a large population. More importantly, these asymptomatic patients have same high communicability but concealment property.6 Therefore, asymptomatic infection is a nonnegligible chain of infection transmission.
Currently, the development of drugs for COVID-19 bot- tleneck has been encountered. Many promising antiviral therapies are reported to have limited effect on hospitalized patients with COVID-19.7 For asymptomatic infection, it is more difficult to intervene because there are no typical symptoms. At present, the recommended medical observation period for COVID-19 patients in incubation period is up to 14 days.8 Without effective treatment, these patients are of very large probability to develop into clinically confirmed cases. Traditional Chinese Medicine (TCM) played an important role in the COVID-19 epidemic in China as complementary and alternative medicine.9–11 Lianhua Qingwen (LH) capsule is a patent TCM drug for treating COVID-19, officially re- commended by the National Health Commission of the Peo- ple’s Republic of China. It has confirmed the effectiveness on COVID-19-infected patients with mild, common, and severe symptoms.12–15 However, whether it provides significant benefit to asymptomatic patients needs to be validated.
In this trial, the authors conducted a randomized, con- trolled multicenter trial, aiming to explore the effectiveness and safety of LH capsule in treating asymptomatic COVID- 19 patients. Considering the short and need of therapeutic methods for asymptomatic patients, this study may provide more evidence that supports LH capsule as a potential option in clinical.
Methods
Study design
This was a randomized, controlled multicenter trial of asymptomatic COVID-19 patients who were positive in
PCR test but showed no typical symptoms. In total, 120 patients were included in this trial and randomly divided into treatment group and control group. The study was ap- proved by the ethics committee of Hebei Chest Hospital (No. 2021003). Good Clinical Practice (GCP) guidelines and the Declaration of Helsinki were strictly followed. The study has been registered in Chinese Clinical Trial Registry. Written informed consent has been obtained from the pa- tients or legal representatives. CONSORT Checklist of in- formation to include when reporting a randomized trial is listed in Supplementary S1.
Patients
The inclusion criteria were as follows: (1) patients asymptomatically infected with novel coronavirus pneu- monia discovered through pathogenic testing; (2) older than 18 years (including 18 years old); (3) voluntarily sign a written informed consent before the beginning of the study. The exclusion criteria were as follows: (1) patients with new coronavirus pneumonia confirmed by pathogenic testing; (2) in the opinion of the investigator, patients with serious diseases such as malignant disease, autoimmune disease, liver and kidney disease, blood disease, neurological dis- ease, and endocrine disease may affect patients’ participa- tion in the trial or influence the outcome of the study; (3) pregnant or lactating women; (4) patients who participated in other clinical trials within the last 3 months; (5) an al- lergic condition, such as a history of allergies to two or more drugs or foods, or a known allergy to the ingredients of the drug; (6) the investigator believes that there are any factors that are not suitable for enrollment or affect the evaluation of the effectiveness.
In total, 120 patients from three hospitals (Hebei Chest Hospital, the Second Hospital of Xingtai, and Harbin In- fectious Diseases Hospital) were included in this trial during January 1 to March 31, 2021. None of the patients were vaccinated. Visit was performed at day 0, 7, and 14.
Clinical classifications
All patients were asymptomatic at the beginning of the trial. At the endpoint of the trial, patients were classified into four types, including asymptomatic, mild, common, and severe cases. Asymptomatic: confirmed cases with no clin- ical symptoms; Mild: confirmed cases with fever (measured or subjective) or respiratory symptoms; Common: confirmed cases with fever (measured or subjective) or respiratory symptoms, and radiographic evidence of pneumonia; Se- vere: confirmed cases with evidence including fever, respi- ratory symptoms, radiographic evidence of pneumonia, and at least one of the following symptoms: (1) respiratory distress, respiration rate of ‡30 times/min; (2) resting-state, mean oxygen saturation of £93%; (3) PaO2/FiO2 £300 mmHg (1 mmHg = 0.133 kPa).
Sample size calculation
The main purpose of this study was to investigate the negative conversion rate of COVID-19 nucleic acid with or without LH capsule treatment. The authors assumed that the negative rate of the treatment group was 50% and that of the control group was 25% according to the clinical experience in China. The patients in the treatment group and the control group were allocated in the ratio of 1:1 (a = 0.05 [bilateral] and power = 0.80), and the total sample size was 110 cases according to Power Analysis and Sample Size 15.0 calcu- lation. Assuming that the dropout rate was <10%, the total sample size of this study was finally set to 120, including 60 cases in the treatment group and 60 cases in the control group.
Randomization and grouping
Block randomization method was used in this trial, and randomization numbers were produced by using the SAS 9.4 software (Order No. 9C1XJD; SAS Institute, Cary, NY). A total of 120 patients were divided into the treatment group and the control group. The computer-based 1:1 block ran- domization method was utilized to assign cases to the treatment group and the control group, respectively. The block length of the randomization was 4. The randomization list was kept by the statisticians. To ensure the allocation concealment, the detail of randomization was distributed to the clinicians by using sequentially numbered, opaque sealed envelopes.
Each consecutively coded patient was randomly recruited and numbered by the clinicians in order until the pre- supposed number of cases reached. All attending clinicians have obtained the qualification of clinical trial from the State Drug Administration. Third-party data analysis was performed independently by professional statisticians from Huazhong University of Science and Technology. Both the statisticians and outcome assessors were unaware of the grouping.
Study medication
For the control group, participants were required isola- tion according to the Diagnosis and Treatment Program for Novel Coronavirus Infection Pneumonia (Trial Eighth Edition) released by the National Health Commission of China.16 LH capsules were manufactured based on the Pharmacopedia of People’s Republic of China. The major ingredients of LH are as follows: Lonicera japonica, For- sythia suspensa, Rheum palmatum, Isatis indigotica, Ephe- dra sinica, Pogostemon cablin, Dryopteris crassirhizoma, Glycyrrhiza uralensis, Rhodiola crenulata, Prunus sibirica, Houttuynia cordata, and gypsum. For the treatment group, patients were isolated and orally took LH capsule (batch No. B2012037, 0.35 g per capsule, 4 capsules, thrice daily) for
14 days. Once developing into clinical confirmed cases,
participants were transferred to routine medical treatment in hospital and recorded in trial data.
Endpoints
The primary endpoints were the time and rate of nu- cleic acid turning negative during the isolation observa- tion period according to PCR test (batch No.: 20040999; DAAN Gene, Guangzhou, China). The secondary end- points included the clinical symptoms and severity, clinical symptoms appearance time and proportion, pro- portion of mild and common cases of novel coronavirus pneumonia diagnosed during the isolation observation period, routine blood test, and biochemical indicators,according to the Diagnosis and Treatment Protocol for COVID-19 Patients (Trial Eighth Edition) (Supple- mentary File S2).
Safety
Adverse events (AEs) occurring during the trial, with or without causal association with the study drug, were re- corded.
Statistical analyses
All statistical analyses were conducted with the SAS 9.4 software (Order No. 9C1XJD; SAS Institute). The main outcomes were measured and assessed by using the full analysis set (FAS), which included all randomly assigned patients. A per-protocol set (PPS) analysis limited to pa- tients who followed the protocol and completed the trial was also conducted. For descriptive analysis, counting data is described by the number of cases and composition ratio. Measurement data are described by mean, standard devia- tion, maximum, and minimum. Nonnormally distributed data are described by median and 25th and 75th percentiles. For effectiveness analysis, the rate of nucleic acid turning negative was tested for superiority compared with the con- trol group, and the 95% confidence interval (CI) of the rate difference was calculated by the Newcombe–Wilson meth- od. If the lower limit of the 95% CI is greater than 0, it can be considered effective established. The time for nucleic acid to be negative was compared by log-rank test.
Safety analysis (safety set) was used to perform the safety evaluation. Descriptive statistics of the AEs occurred in this study was performed. The number of patients with AEs and adverse reactions in each group and their percentages were listed. The incidence of AEs between the groups was com- pared using the w2 test or Fisher’s exact probability method.
Results
Patients characteristics
The flowchart of the trial is presented in Figure 1. Totally,
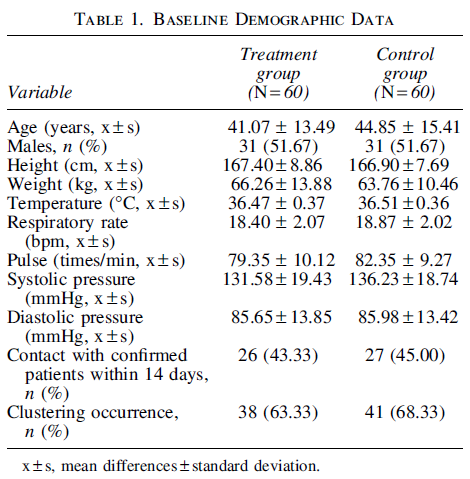
120 asymptomatic COVID-19 cases were included and randomized in this trial from January 1 to March 31, 2021, with 60 each in the control and treatment groups. No par- ticipant withdrew from the trial early and permanently. Both groups were comparable in age, sex, physicality, tempera- ture, and epidemiology statistics at onset (Table 1).
Primary endpoints
The rate of nucleic acid turning negative at 14 days was higher in the treatment group compared with the control group (FAS: 48.33% vs. 26.67%, rate difference: 21.66%,
95% CI: 4.34 to 37.27, p = 0.0142; PPS same as FAS)
(Table 2). Meanwhile, the time for nucleic acid turning negative in the treatment group was shorter in comparison with that in the control group (FAS: 7.5 vs. 14.5 days, p = 0.018) (Fig. 2).
Secondary endpoints
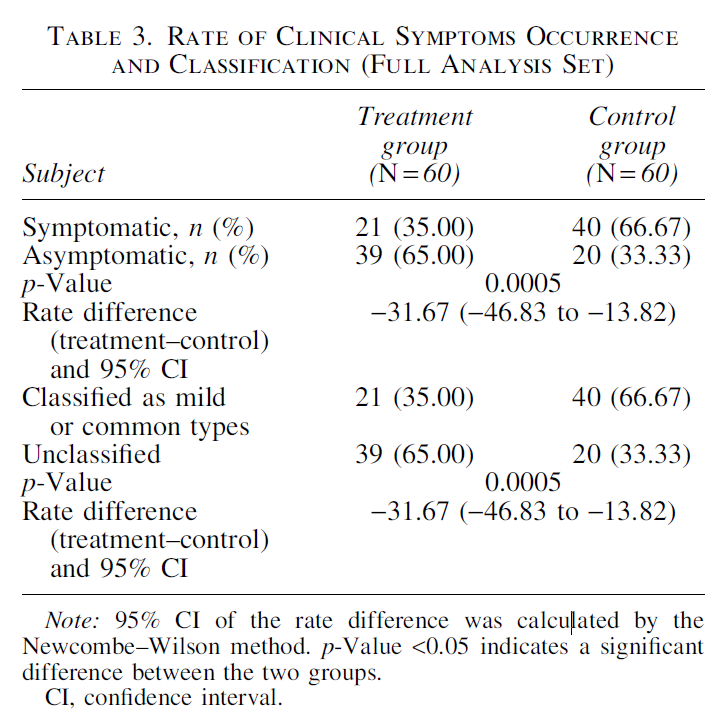
The proportion of clinical symptoms appearance during the isolation observation period was smaller in the treatment group in comparison with the control group (FAS: 35.00%
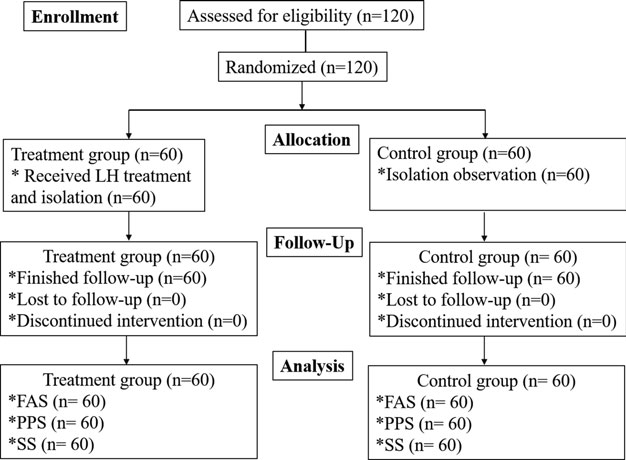
FIG. 1. Study flowchart. FAS, full analy- sis set; LH, Lianhua Qingwen; PPS, per- protocol set; SS, safety set.
vs. 66.67%, rate difference: -31.67, 95% CI: -46.83 to -13.82, p = 0.0005). In addition, the time of clinical symptoms appearance was longer in the treatment group (Fig. 3; FAS: 6.0 days vs. 2.0 days, p < 0.0001). Compared with the control group, few patients developed into ild type (FAS:6.67% vs. 8.33%) or common type (FAS: 28.33% vs.58.34%) in the treatment group (Table 3).
Compared with the control group, the incidence rate of fever during isolation observation was lower in the treatment group (FAS: 6.67% vs. 30.00%, p = 0.0010). The incidence rate of fatiguewas also decreased in the treatment group (FAS: 6.67% vs. 20.00%, p = 0.0317). By analyzing the incidence rate of respiratory symptoms, lower incidence rate of cough (FAS: 23.33% vs. 46.67%, p = 0.0074) and expectoration (FAS: 8.33% vs. 23.33%, p = 0.0074) was observed in the treatment group compared with the control group (Table 4).
Safety
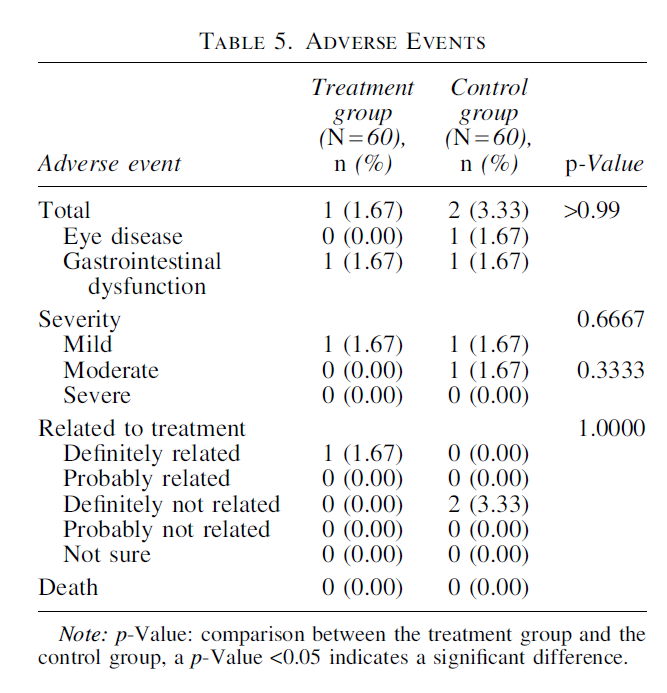
Safety findings are summarized in Table 5. The incidence rates of AEs were similar in both the groups, with 1.67% and 3.33% in the treatment group and the control group, respectively ( p > 0.99). In the treatment group, one patient was reported to have mild gastrointestinal dysfunction and has confirmed relationship to the LH treatment. In the control group, two patients were documented with mild eye disease and moderate gastrointestinal dysfunction, respectively,with no relationship to treatment. No death case was reported in the two groups.
Discussion
The breakout and pandemic of COVID-19 since 2019 have caused far-reaching impact on great change to global society. Medical resources incline to the prevention and treatment to COVID-19 infections. Meanwhile, social contacts turn to long-range or remote forms. According to a transmission dynamics study performed by researchers from Harvard, we have to coexist with SARS-CoV-2 for at least 5 years.2 However, there are no effective interventions or drugs to stop this epidemic. An Interim WHO Solidarity Trial involving 11,330 COVID-19 patients showed that 4 most promising antiviral drugs, including remdesivir, hy- droxychloroquine, lopinavir, and interferon regimens, had little or no effect on hospitalized patients with COVID-19.7 Moreover, a clinical trial from China reported that vaccines for COVID-19 could induce the production of antibodies in the body, but up to about 90% individuals had reduction in IgG and neutralizing antibody levels in asymptomatic and symptomatic infections.17

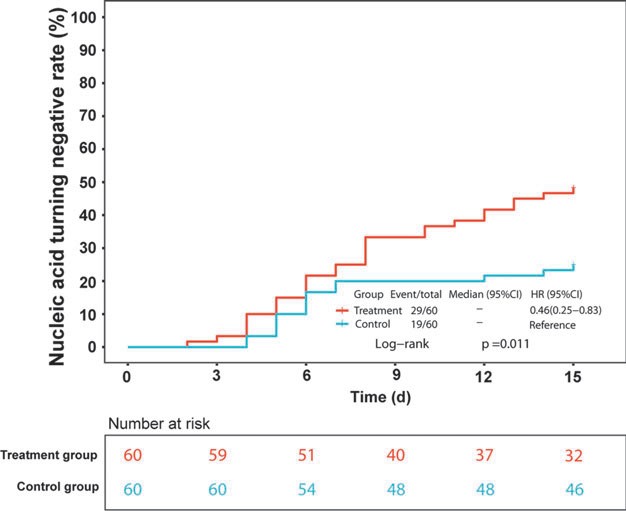
FIG. 2. Dynamic changes of nucleic acid turning negative rate in the FAS. Red and blue lines represent the treatment and con- trol groups, respectively. CI, confidence in- terval; FAS, full analysis set.
Increasing evidence show that asymptomatic patients are of a large proportion in COVID-19 infections. According to recent reports from different countries, about 30%–50% patients are asymptomatic.18–20 More seriously, it has been reported that the viral load in the asymptomatic patient was similar to that in the symptomatic individuals, suggesting a nonnegligible transmission infectivity and potential.21 However, these asymptomatic individuals can easily be ig- nored in epidemic prevention.22 Measures and methods es- tablished for those confirmed in-hospital patients are not applicable to asymptomatic individuals because there is little clinical evidence to support the symptomatic treatment.
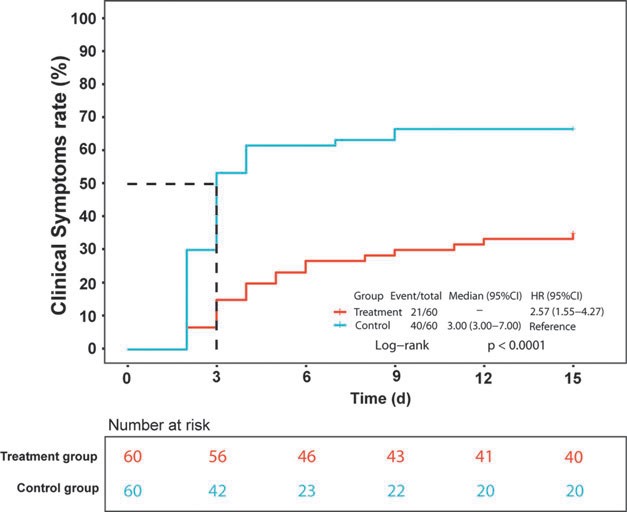
FIG. 3. Dynamic changes of clinical symptoms rate in the FAS. Red and blue lines represent the treatment and control groups, respectively. CI, confidence interval; FAS, full analysis set; HR, hazard ratio.
Due to the less importance and urgency, investment on the research and development of drugs for asymptomatic infection is much scarcer compared with symptomatic in- fections. Therefore, except the isolation observation, only antiviral interventions can be considered as options. How- ever, the treatment of asymptomatic infection is controver- sial. Although it is widely believed that antiviral drugs could fasten the viral clearance in asymptomatic infections,5,23 several recent studies showed that these drugs exhibit lim- ited or no effectiveness in accelerating viral clearance or
symptomatic improvement.24,25
The use of TCM for preventing and treating Wen Yi, also known as epidemic diseases, was first recorded in ancient Chinese practice cited in Huangdi’s Internal Classic. In re- cent years, accumulating evidence-based studies confirmed the effectiveness and safety of TCM in treating infectious diseases, such as malaria,26 SARS,27 and H1N1 influenza.28 In the fight against the COVID-19 epidemic, the application of TCM played an important role in treating infected pa- tients. Mounting evidence revealed that early intervention with TCM is beneficial to the outcome of COVID-19 pa- tients by improving clinical cure rate, relieving symptoms, and reducing mortality rate.9,11,29 LH capsule is a widely used TCM drug recommended by authority organization of Chinese government for treating infectious diseases and approved for phase II clinical trial by the U.S. Food and Drug Administration in 2015.
A report at the early epidemic of COVID-19 showed that
LH capsule could ameliorate clinical symptoms of COVID- 19 patients with mild and common type.13 Considering the lack of drugs and methods for asymptomatic patients, the authors investigated the curative and interruptive effect of LH capsule on these individuals. According to the data of this study, LH treatment could fasten the virus clearance by increasing the rate and shortening the time of nucleic acid turning negative during the isolation observation period.

This is an important pesticide effect for asymptomatic pa- tients, which may contribute to delaying and blocking the disease progression. Actually, it has been reported that LH capsule may block the binding of SARS-CoV-2 with an- giotensin converting enzyme 2 to inhibit replication of the virus and reduce virions in infected cells.30,31
Moreover, the data of this study showed that LH treat- ment may reduce the occurrence of clinical symptoms and eventually decrease the proportion of confirmed mild and common cases converted from asymptomatic patients. Re- cent mechanism researches provided more scientific evi- dence that LH capsule and its active ingredients may bind to several key targets of inflammatory response and tissue damage, including protein kinase B (AKT), interleukin-6, prostaglandin-endoperoxide synthase 2, and mitogen- activated protein kinase 1.32–34 These data explained how LH treatment decreases the appearance of fever, lung in- flammation, and tissue damage in asymptomatic patients. The safety of LH capsule in clinical use is credible since the
present study and many other trials reported little or no AEs.10,13,35
COVID-19 epidemic is now attacking the public health and will continuously influence the society in the future. Asymptomatic patient is a key point of the COVID-19 transmission, with high proportion and infectivity. However, interventions are quite limited at this stage. In this study, the authors suggest that LH capsule may be beneficial to asymptomatic COVID-19 patients and could be considered as a potential choice. However, there are some limitations of this study. The size of this trial is small, and no placebo was implemented, which may affect the scientificity of the conclusion. Besides, due to the lack of research on COVID- 19 asymptomatic infection, the calculation of the sample size of this study is based on clinical experience. With growing understanding of COVID-19 infections, an ex- tended study should be needed to thoroughly explore the effects of LH capsules on asymptomatic COVID-19 pa- tients.
Acknowledgment
The statistical analyses were performed by the School of Public Health, Tongji Medical College, Huazhong Uni- versity of Science and Technology.
Authors’ Contributions
Q.L., J.M., and S.W. designed the trial and provided ad- ministrative support. L.Z., L.W., X.X., Y.Y., R.J., X.Y., X.Z., Y.G., and H.S. provided study materials and collected the information of patients. L.Z., L.W., X.X., J.H., and X.W.
analyzed and interpreted the patient data. L.Z., L.W., and X.X. were major contributors in writing the article. All authors read and approved the final article.
Acknowledgment
The statistical analyses were performed by the School of Public Health, Tongji Medical College, Huazhong Uni- versity of Science and Technology.
Authors’ Contributions
Q.L., J.M., and S.W. designed the trial and provided ad- ministrative support. L.Z., L.W., X.X., Y.Y., R.J., X.Y., X.Z., Y.G., and H.S. provided study materials and collected the information of patients. L.Z., L.W., X.X., J.H., and X.W.
analyzed and interpreted the patient data. L.Z., L.W., and X.X. were major contributors in writing the article. All authors read and approved the final article.
Consent for Publication
The publication of computed tomography manifestation images was approved by the patients. Written informed consent was signed by patients themselves.
Availability of Data and Materials
The data sets used and/or analyzed during the current study are available from the corresponding authors on reasonable request.
The publication of computed tomography manifestation images was approved by the patients. Written informed consent was signed by patients themselves.
Availability of Data and Materials
The data sets used and/or analyzed during the current study are available from the corresponding authors on reasonable request.
Author Disclosure Statement
The authors declare that they have no competing interests.
Funding Information
This study was funded by the Key Program of the National Natural Science Foundation of China (Grant No. 82130123),S&T Program of Hebei (Grant No. 206Z2503G), and the National Major Scientific and Technological Project (Grant No. 2017ZX10305501).
Supplementary Material
Supplementary S1
Supplementary File S2
References
1. Chan JF, Yuan S, Kok KH, et al. A familial cluster of pneumonia associated with the 2019 novel coronavirus indicating person-to-person transmission: A study of a family cluster. Lancet 2020;395:514–523.
2. Kissler SM, Tedijanto C, Goldstein E, et al. Projecting the transmission dynamics of SARS-CoV-2 through the postpandemic period. Science 2020;368:860–868.
3. Fineberg HV. Ten weeks to crush the curve. N Engl J Med 2020;382:e37.
3. Fineberg HV. Ten weeks to crush the curve. N Engl J Med 2020;382:e37.
4. Tian S, Hu N, Lou J, et al. Characteristics of COVID-19 infection in beijing. J Infect 2020;80:401–406.
5. Hu Z, Song C, Xu C, et al. Clinical characteristics of 24 asymptomatic infections with COVID-19 screened among close contacts in Nanjing, China. Sci China Life Sci 2020;63:706–711.
6. Sah P, Fitzpatrick MC, Zimmer CF, et al. Asymptomatic SARS-CoV-2 infection: A systematic review and metaanalysis. Proc Natl Acad Sci U S A 2021;118:e2109229118.
7. WHO Solidarity Trial Consortium, Repurposed Antiviral Drugs for Covid-19—Interim WHO Solidarity Trial Results. N Engl J Med 2021;384:497–511.
8. Hoang VT, Dao TL, Gautret P. Recurrence of positive SARS-CoV-2 in patients recovered from COVID-19. J Med Virol 2020;92:2366–2367.
9. Chen G, Su W, Yang J, et al. Chinese Herbal Medicine reduces mortality in patients with severe and critical coronavirus disease 2019: A retrospective cohort study. Front Med 2020;14:752–759.
10. Shi N, Guo L, Liu B, et al. Efficacy and safety of Chinese Herbal Medicine versus lopinavir-ritonavir in adult patients with coronavirus disease 2019: A non-randomized controlled trial. Phytomedicine 2021;81:153367.
11. An X, Zhang Y, Duan L, et al. The direct evidence and mechanism of Traditional Chinese Medicine treatment of COVID-19. Biomed Pharmacother 2021;137:111267.
12. Liu M, Gao Y, Yuan Y, et al. Efficacy and safety of integrated Traditional Chinese and Western Medicine for corona virus disease 2019 (COVID-19): A systematic review and meta-analysis. Pharmacol Res 2020;158:104896.
13. Hu K, Guan WJ, Bi Y, et al. Efficacy and safety of Lianhuaqingwen capsules, a repurposed Chinese herb, in patients with coronavirus disease 2019: A multicenter,prospective, randomized controlled trial. Phytomedicine 2021;85:153242.
14. Li LC, Zhang ZH, Zhou WC, et al. Lianhua Qingwen prescription for coronavirus disease 2019 (COVID-19) treatment: Advances and prospects. Biomed Pharmacother 2020;130:110641.
15. Li S, Zhang J, Li F, et al. Traditional Chinese Medicine Lianhua Qingwen for treating COVID-19: A protocol for a meta-analysis and systematic review of randomized controlled trials. Medicine (Baltimore) 2021;100:e24204.
16. Diagnosis and Treatment Program for Novel Coronavirus Infection Pneumonia (Trial Eighth Edition). 2021. Available from: http://www.nhc.gov.cn/yzygj/s7653p/202104/ 7de0b3837c8b4606a0594aeb0105232b.shtml.
17. Long QX, Tang XJ, Shi QL, et al. Clinical and immunological assessment of asymptomatic SARS-CoV-2 infections.Nat Med 2020;26:1200–1204.
18. Nishiura H, Kobayashi T, Miyama T, et al. Estimation of the asymptomatic ratio of novel coronavirus infections (COVID-19). Int J Infect Dis 2020;94:154–155.
19. Wu J, Liu X, Zhou D, et al. Identification of RT-PCRnegative asymptomatic COVID-19 patients via serological testing. Front Public Health 2020;8:267.
20. Rivett L, Sridhar S, Sparkes D, et al. Screening of healthcare workers for SARS-CoV-2 highlights the role of asymptomatic carriage in COVID-19 transmission. Elife 2020;9:e58728.
21. Zou L, Ruan F, Huang M, et al. SARS-CoV-2 viral load in upper respiratory specimens of infected patients. N Engl J Med 2020;382:1177–1179.
22. Qiu J. Covert coronavirus infections could be seeding new outbreaks. Nature 2020; doi: 10.1038/d41586-020-00822-x
23. Tao PY, Leng L, Liu K, et al. Determination of risk factors for predicting the onset of symptoms in asymptomatic COVID-19 infected patients. Int J Med Sci 2020;17:2187–2193.
24. Doi Y, Hibino M, Hase R, et al. A prospective, randomized,open-label trial of early versus late favipiravir therapy in hospitalized patients with COVID-19. Antimicrob Agents Chemother 2020;64:e01897-20. 25. Hua CZ, Miao ZP, Zheng JS, et al. Epidemiological features
and viral shedding in children with SARS-CoV-2infection. J Med Virol 2020;92:2804–2812.
26. Pinheiro L, Feitosa LM, Silveira F, et al. Current antimalarial therapies and advances in the development of semisynthetic artemisinin derivatives. An Acad Bras Cienc 2018;90(1 Suppl. 2):1251–1271.
27. Chen Z, Nakamura T. Statistical evidence for the usefulness of Chinese medicine in the treatment of SARS. Phytother Res 2004;18:592–594.
28. Wang C, Cao B, Liu QQ, et al. Oseltamivir compared with the Chinese traditional therapy maxingshigan-yinqiaosan in the treatment of H1N1 influenza: A randomized trial. Ann Intern Med 2011;155:217–225.
29. Ren JL, Zhang AH, Wang XJ. Traditional Chinese medicine for COVID-19 treatment. Pharmacol Res 2020;155:104743.
30. Niu M, Wang RL, Wang ZX, et al. Rapid establishment of traditional Chinese medicine prevention and treatment of 2019-nCoV based on clinical experience and molecular docking. Zhongguo Zhong Yao Za Zhi 2020;45:1213–1218.
31. Runfeng L, Yunlong H, Jicheng H, et al. Lianhuaqingwen exerts anti-viral and anti-inflammatory activity against novel coronavirus (SARS-CoV-2). Pharmacol Res 2020;156:104761.
32. Niu WH, Wu F, Cao WY, et al. Network pharmacology for the identification of phytochemicals in Traditional Chinese Medicine for COVID-19 that may regulate interleukin-6. Biosci Rep 2021;41:BSR20202583.
33. Shen X, Yin F. The mechanisms and clinical application of traditional Chinese medicine Lianhua-Qingwen capsule.Biomed Pharmacother 2021;142:111998.
34. Xia QD, Xun Y, Lu JL, et al. Network pharmacology and molecular docking analyses on Lianhua Qingwen capsule indicate Akt1 is a potential target to treat and prevent COVID-19. Cell Prolif 2020;53:e12949.
35. Zhao P, Yang HZ, Lv HY, et al. Efficacy of Lianhuaqingwen capsule compared with oseltamivir for influenza a virus infection: A meta-analysis of randomized, controlled trials. Altern Ther Health Med 2014;20:25–30.
Address correspondence to:
Qingquan Liu, MD
Intensive Care Unit
Beijing Hospital of Traditional Chinese Medicine
Capital Medical University
23 Meishuguan Backstreet
Dongcheng, Beijing 100010
P.R. China
E-mail: liuqingquan_2003@126.com
Jianqiang Mei, MD
Respiratory Department
Hebei Hospital of Traditional Chinese Medicine
389 Zhongshan East Street
Changan, Shijiazhuang 050011
P.R. China
E-mail: mjq1000000@sina.com
Shucai Wu, MD
Respiratory Department
Hebei Chest Hospital
372 Shengli North Street
Changan, Shijiazhuang 050041
P.R. China
E-mail: shucaiwu2009@163.com
(责任编辑:张云文)